SBAR is a standardized way of communicating with other healthcare givers. It promotes patient safety because it helps physicians and nurses communicate with each other. Staff and physicians can use SBAR to share what information is important about a patient. It improves efficiency because this standardized form of communication helps caregivers speak about patients in a concise and complete way. It is also mandated by the Joint Commision on Accrediation of Hospital Organization which has added to Goal 2 in the 2007 Patient Safety Goals. The additional statement (2e) reads, “Implement a standardized approach to “hand off” communications, including an opportunity to ask and respond to questions.”SBAR is an acronym that stands for:Situation
Background Assessment Recommendation Using SBAR, patient reports are more accurate, efficient, and consistent enterprise-wide. This simple, yet highly effective communication technique can be used when:-A nurse is calling a physician -Nurses are handing off patients to one another -Nurses are transferring patients to other facilities or to other levels of careSBAR promotes better communication. In most cases nurses and physicians communicate in very different ways. Nurses are taught to report in narrative form, providing all details known about the patient. Physicians are taught to communicate in using brief “bullet points” that provide key information to the listener.This is the form on how Nurse's should report to a physician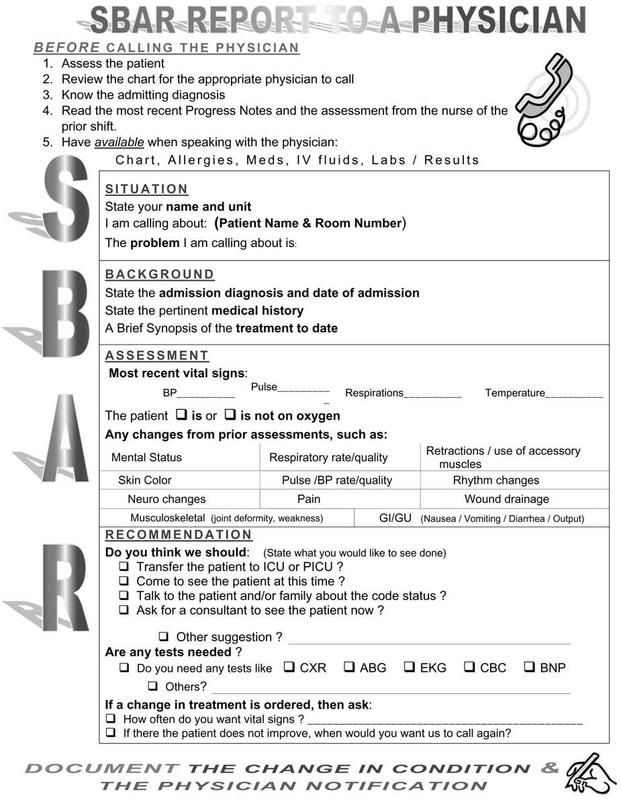 Here is an example of how to use the template:
Here is an example of how to use the template:
Dr. Jones, this is Jedz Cutie RN, I am calling from PBSN Hospital about your patient Mr. D. Bitteroot.
Situation: Here's the situation: Mr. Bitteroot is having increasing dyspnea and is complaining of chest pain.
Background: The supporting background information is that he had a total knee replacement two days ago. About two hours ago he began complaining of chest pain. His pulse is 120 and his blood pressure is 128/54. He is restless and short of breath
Assessment: My assessment of the situation is that he may be having a cardiac event or a pulmonary embolism.
Recommendation: I recommend that you see him immediately and that we start him on 02 stat.
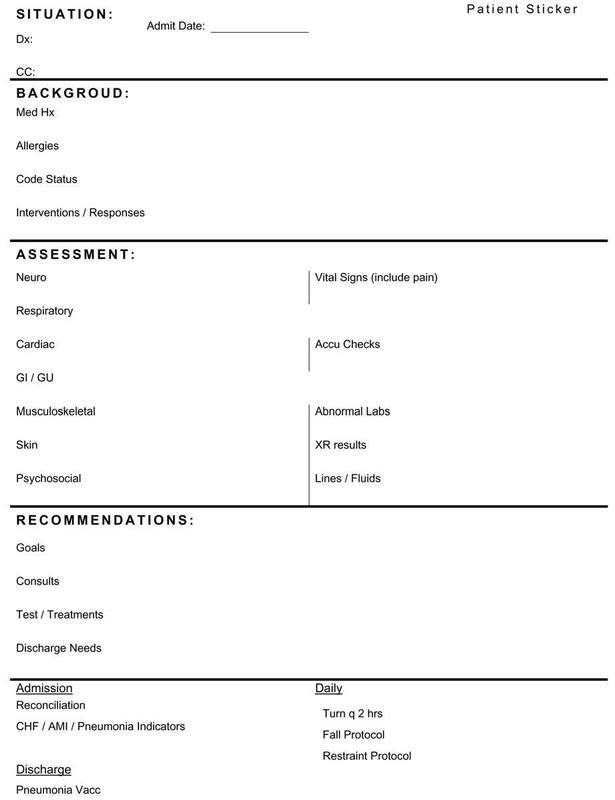
Another form that is used is the Hand-off form which can be used for exchange of shift report used by nurse to nurse communication.
REFERENCE: Kathleen M. Haig, R.N., Staci Sutton, R.N., John Whittington, M.D. "SBAR: A Shared Mental Model for Improving Communication Between Clinicians" Joint Commision on Quality and Patient Safety www.jcipatientsafety.org/fpdf/psp/SBAR.pdf (Last Accessed, May 25, 2008)














